Incisional/Ventral Hernia Surgery
What is a Hernia?
A hernia is the protrusion of part of an organ through an opening in the abdominal wall or an opening within the abdominal cavity. It can either be developed at birth (congenital) or it may appear later in life (acquired).
There are natural openings in the wall of the abdomen or within the abdominal cavity that allows certain structures to pass through.
In an acquired hernia, connective tissue degenerates through the process of aging which allows either existing natural openings to widen or new defects to develop in the abdominal wall. This is mediated through increase in pressure inside the abdomen leading to a bulge or protrusion of an internal organ out of the abdomen. Some of the factors that contribute to the development of a hernia through the chronic increase in pressure are persistent coughing, obesity, constipation, and frequent heavy lifting. Herniae are also more common in pregnancy, smokers, previous abdominal surgery, and in certain connective tissue disorders.
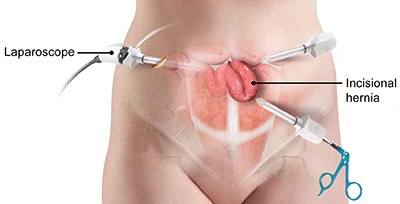
Incisional hernia- is a type of hernia that occurs as a result of weakening of the abdominal wall tissue caused by a previous surgical incision. Although sound abdominal wall closure techniques reduce the risk of developing incisional herniae in the future, body tissue in a fully healed surgical incision site is never as strong as tissue that has never had surgery previously.
Ventral hernia- is a type of hernia that is located along the midline in any part of the abdominal wall.
Symptoms
Symptoms depend on the contents of the hernia and whether it can be pushed back inside the abdomen (reducibility).
If the hernia contains protrusion of fat, then it may only cause pain. If the hernia contains bowel that cannot be pushed back in, then it may cause pain, bowel obstruction, and gangrenous bowel in the protruding segment. This situation is a surgical emergency that requires an urgent operation.
Diagnosis
Diagnosis of these conditions primarily involve in review of medical history and a thorough physical examination to identify the hernia, its likely contents and whether they can be reduced back into the abdominal cavity. An abdominal x-ray may be ordered to confirm or rule out an associated bowel obstruction. In some situations, an abdominal CT scan may be performed for surgical planning if there is a clinical suspicion of multiple incisional/ventral herniae.
Treatment
Hernia containing irreducible bowel/fat requires urgent surgical consultation in the hospital.
In the non-emergency setting, surgery is usually recommended for symptomatic hernia or those containing bowel in the hernia. It may also be performed for the undesirable cosmesis of a hernial bulge.
Depending on a number of factors (including number, site and size of herniae), the surgical approach of either an open hernia repair (with a larger incision) or laparoscopic (key-hole) repair would be recommended.
The operation commonly involves in the use of synthetic material (a mesh) to repair the abdominal wall defect using “tension-free” principles to reduce the risk of hernia recurrence after surgery. The mesh provides a scaffold for the incorporation and integration of scar tissue.